Need to convert IV Solumedrol to oral prednisone? A general equivalent is approximately 5 mg of prednisone for every 1 mg of Solumedrol. However, this is a rough guideline; individual responses vary significantly.
Dosage adjustments are crucial. Factors influencing the conversion include patient weight, disease severity, and individual metabolic rates. Always consult a physician for precise dosage calculations tailored to the specific patient’s needs. They will account for these factors and other relevant medical history.
Remember: This information is for educational purposes only and does not constitute medical advice. Do not attempt to self-medicate or alter your prescribed treatment plan without direct supervision from a qualified healthcare professional. Accurate conversion requires clinical judgment and individual assessment.
- Iv Solumedrol Oral Prednisone Equivalent: A Detailed Comparison
- Understanding Solumedrol (Methylprednisolone)
- Understanding Oral Prednisone
- Dosage Equivalents: A Complex Calculation
- Factors Influencing Conversion
- Recommendations and Cautions
- Pharmacokinetic Differences: Absorption and Metabolism
- Clinical Scenarios Requiring Conversion
- Acute Exacerbation Management
- Chronic Inflammatory Conditions
- Dosage Adjustments
- Considerations for Conversion: Patient Factors and Disease States
- Specific Disease States
- Patient-Specific Adjustments
- Monitoring and Follow-up
- Potential Side Effects and Management
- Gastrointestinal Issues
- Fluid Retention and Hypertension
- Mood Changes and Insomnia
- Other Potential Effects
- Important Note
- When to Consult a Physician: Importance of Medical Guidance
- Medication Interactions and Adjustments
- Monitoring Your Progress
- Specific Symptoms Requiring Immediate Attention
Iv Solumedrol Oral Prednisone Equivalent: A Detailed Comparison
There’s no single, universally agreed-upon conversion factor between intravenous methylprednisolone (Solumedrol) and oral prednisone. Dosage depends heavily on the specific condition being treated, patient factors, and physician preference. However, we can offer some general guidelines.
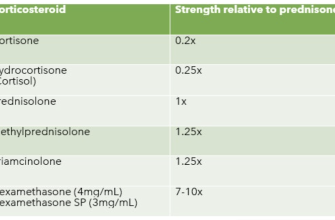
Many clinicians use a rough equivalence of 5mg of oral prednisone to 1mg of intravenous methylprednisolone. This is a starting point, and adjustments are often necessary.
- Example 1: A patient receiving a single 1000mg IV dose of Solumedrol might transition to an equivalent oral prednisone dosage regimen starting around 200mg daily, gradually tapered down over several days or weeks.
- Example 2: A patient on a Solumedrol IV infusion might transition to a significantly lower daily dose of oral prednisone, possibly even less than the simple 5:1 conversion would suggest. This often depends on the duration of IV therapy and clinical response.
Factors influencing the conversion include:
- Disease Severity: More severe conditions might necessitate higher oral prednisone doses for equivalent impact.
- Patient Metabolism: Individual differences in how the body processes medication influence the required dosage.
- Duration of Treatment: Short-term IV Solumedrol often requires different conversion calculations than prolonged treatment.
- Clinical Response: Dosage adjustment is crucial based on how the patient responds to therapy. Blood tests and clinical symptoms guide physicians.
Crucially: This information is for general knowledge and shouldn’t guide medical decisions. Always consult a healthcare professional for appropriate medication adjustments. They’ll consider the individual’s needs and clinical picture to determine the best course of action and safest conversion strategy.
Disclaimer: This content is for informational purposes only and does not constitute medical advice. Always consult with a qualified healthcare professional for any health concerns or before making any decisions related to your health or treatment.
Understanding Solumedrol (Methylprednisolone)
Solumedrol, the brand name for methylprednisolone, is a corticosteroid medication. It’s a powerful anti-inflammatory drug, meaning it reduces swelling and inflammation throughout the body.
Doctors prescribe Solumedrol for various conditions, including severe allergic reactions, asthma attacks, and autoimmune diseases. It’s often administered intravenously (IV) for rapid action in emergencies.
Methylprednisolone’s effects are potent, acting by suppressing the immune system. This means it’s highly effective against inflammation but also carries potential side effects. These can include increased blood sugar, weight gain, and mood changes. Longer-term use can lead to more serious side effects, so close monitoring is crucial.
The dosage of Solumedrol depends entirely on the individual’s condition and response to treatment. Your doctor determines the appropriate dose and duration. Never adjust your dosage without consulting your physician.
Solumedrol’s IV administration offers quicker relief compared to oral prednisone. However, oral prednisone can provide sustained treatment. The conversion between IV Solumedrol and oral prednisone varies greatly and depends on factors like individual metabolism and the specific condition being treated. Therefore, only a medical professional can accurately determine the equivalent dose.
Remember to discuss potential drug interactions with your doctor or pharmacist. Solumedrol can interact with other medications, potentially affecting their efficacy or increasing side effects.
Always follow your doctor’s instructions precisely. If you experience any concerning side effects, contact your doctor immediately.
Understanding Oral Prednisone
Prednisone is a corticosteroid, meaning it mimics the effects of cortisol, a hormone your body naturally produces. It powerfully reduces inflammation and suppresses your immune system.
Dosage and Administration: Your doctor will determine the precise dose based on your specific needs and condition. Always follow their instructions carefully. Prednisone comes in tablet form and is typically taken orally, once or twice daily, usually with food to minimize stomach upset.
- Never alter your dosage without consulting your doctor. Sudden changes can have serious consequences.
- Take medication at the same time each day to maintain consistent blood levels.
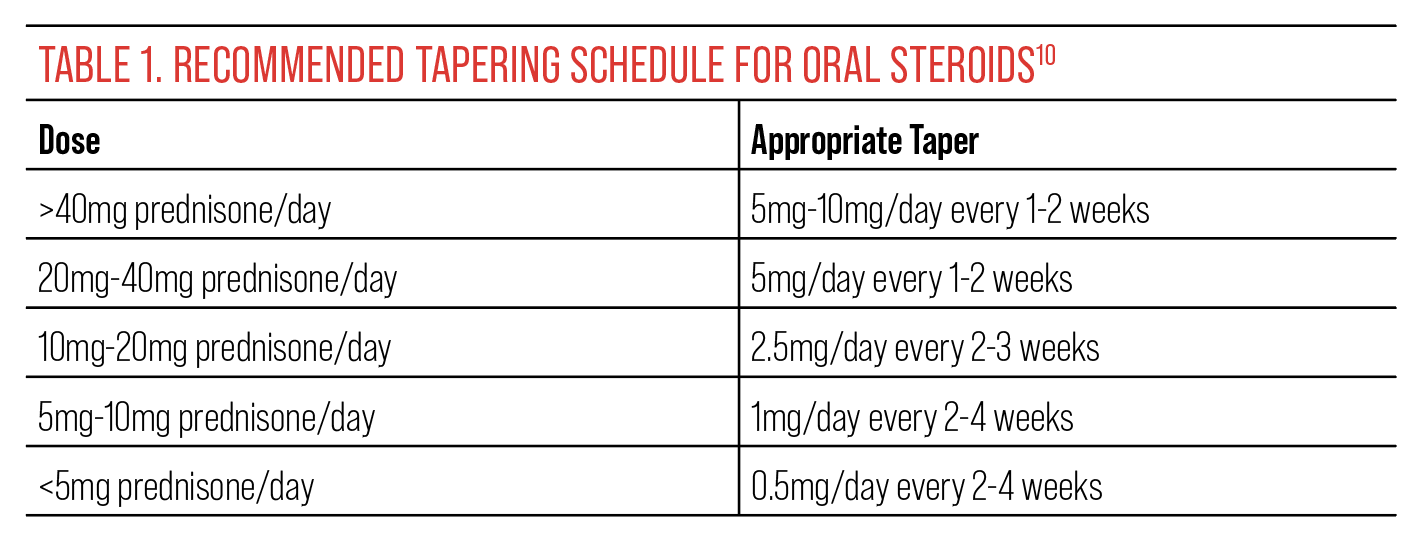
- Don’t abruptly stop taking prednisone. Your doctor will help you gradually reduce your dose to prevent withdrawal symptoms.
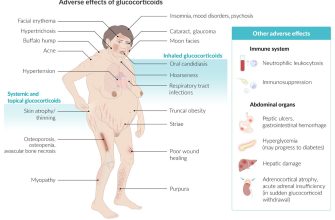
Potential Side Effects: Prednisone can cause a range of side effects, varying in severity depending on dosage and duration of treatment. These include:
- Increased appetite and weight gain
- Mood changes (irritability, anxiety, depression)
- Increased blood sugar
- High blood pressure
- Muscle weakness
- Osteoporosis (weakening of bones)
- Increased risk of infection
- Fluid retention (swelling)
Managing Side Effects: Regular monitoring by your physician is crucial. They can adjust your dosage or prescribe additional medication to manage side effects. A healthy diet, regular exercise, and stress management techniques can also be beneficial.
Interactions: Prednisone can interact with many other medications. Always inform your doctor about all medications, supplements, and herbal remedies you’re taking.
- Discuss potential drug interactions before starting prednisone.
- Provide a complete list of medications to your doctor and pharmacist.
Monitoring: Regular blood tests and check-ups are usually necessary to monitor your progress and detect any potential problems early. Closely observe yourself for any unusual symptoms and report them to your doctor immediately.
Dosage Equivalents: A Complex Calculation
There’s no single, universally accepted conversion factor between intravenous methylprednisolone (Solu-Medrol) and oral prednisone. Conversion depends on several factors including the patient’s individual response, the specific condition being treated, and the route of administration. While some sources suggest a rough 5:1 ratio (5mg methylprednisolone IV to 1mg prednisone orally), this is an oversimplification and should not be used for precise dose calculations.
Factors Influencing Conversion
Consider these variables: The duration of IV methylprednisolone treatment impacts the equivalent oral dose. A short course requires a different calculation than long-term treatment. Also, the disease process itself greatly influences the required dose. Autoimmune diseases, for example, may need higher prednisone maintenance doses compared to inflammatory conditions.
Recommendations and Cautions
Always consult prescribing information and relevant clinical guidelines for specific drug dosing recommendations. Relying solely on conversion ratios without medical oversight is unsafe. Always work with a healthcare professional to develop a safe and effective transition plan between intravenous and oral corticosteroids. Close monitoring of the patient’s response is critical, especially during the transition phase. Adjustments may be needed based on clinical signs and symptoms.
Pharmacokinetic Differences: Absorption and Metabolism
Methylprednisolone (Solu-Medrol) and prednisone differ significantly in their absorption and metabolism. Solu-Medrol, administered intravenously, boasts near-complete bioavailability, bypassing the first-pass metabolism in the liver. This leads to rapid onset of action.
Conversely, oral prednisone undergoes significant first-pass metabolism. This reduces the amount of active drug reaching systemic circulation. Consequently, higher oral prednisone doses are typically required to achieve equivalent therapeutic effects compared to intravenous methylprednisolone.
The metabolism of both drugs primarily involves hepatic reduction to inactive metabolites. However, the rate of this metabolism varies between individuals. This can influence the duration and intensity of their effects. Factors like age, liver function, and concurrent medications can impact these metabolic processes.
| Characteristic | Solu-Medrol (IV Methylprednisolone) | Oral Prednisone |
|---|---|---|
| Absorption | Near-complete bioavailability | Significant first-pass metabolism, reduced bioavailability |
| Onset of Action | Rapid | Slower |
| Metabolism | Hepatic reduction to inactive metabolites | Hepatic reduction to inactive metabolites |
| Dosage Equivalence | Lower doses often needed for similar therapeutic effect | Higher doses typically required |
Consult relevant prescribing information for precise dose adjustments and individual patient considerations. Remember to monitor patients closely for therapeutic response and potential side effects.
Clinical Scenarios Requiring Conversion
Methylprednisolone (Solu-Medrol) and prednisone are both glucocorticoids, but their pharmacokinetic profiles differ significantly. Conversion is necessary when switching between intravenous methylprednisolone and oral prednisone, particularly during transitions between acute and maintenance therapies. Accurate conversion ensures consistent glucocorticoid effects.
Acute Exacerbation Management
Consider a patient with an acute asthma exacerbation initially treated with intravenous Solu-Medrol. Upon improvement, transitioning to oral prednisone requires a conversion factor. A common approach involves using a 5:1 ratio; for example, 125 mg IV methylprednisolone equates to approximately 25 mg oral prednisone daily. This ratio, however, is an approximation; individual patient factors like kidney and liver function influence the actual dose.
Chronic Inflammatory Conditions
Patients with chronic conditions like lupus or rheumatoid arthritis often require long-term glucocorticoid therapy. A similar conversion approach may be used when switching between IV Solu-Medrol and oral prednisone. However, tapering the prednisone dose gradually is crucial to avoid adrenal insufficiency. Close monitoring and adjustments are necessary throughout the transition process.
Dosage Adjustments
Precise conversion ratios lack universal agreement, requiring clinical judgment. Patient age, disease severity, and individual responses all affect optimal dosage. Physicians should consider these factors to determine the appropriate prednisone equivalent. Always prioritize close monitoring of patient response and adjust the oral prednisone dose accordingly.
Considerations for Conversion: Patient Factors and Disease States
Begin by carefully assessing the patient’s individual needs. Age significantly impacts medication metabolism and response. Older adults may require lower doses of prednisone compared to younger patients. Similarly, renal and hepatic function influence drug clearance; reduced function necessitates dose adjustments to avoid toxicity. Always check for concurrent medications, as interactions can affect efficacy and safety.
Specific Disease States
Conversion protocols vary depending on the underlying disease. For example, patients with autoimmune disorders like rheumatoid arthritis might require a more gradual transition to oral prednisone to minimize flare-ups. Conversely, those with acute exacerbations of asthma or allergic reactions may benefit from a quicker switch to reduce symptoms rapidly. Consult established guidelines for specific diseases to determine appropriate conversion strategies.
Patient-Specific Adjustments
Weight influences drug dosage. Comorbidities such as heart disease or diabetes can limit medication choices. Patient preferences and previous experience with corticosteroids must also factor into the decision-making process. Regular monitoring of adverse effects, such as increased blood glucose or fluid retention, is vital for safe and effective conversion.
Monitoring and Follow-up
Close monitoring is necessary throughout the transition. Frequent blood tests can assess for improvements in inflammatory markers and potential side effects. Adjustments in prednisone dosage may be needed based on clinical response and laboratory results. Schedule regular follow-up appointments to evaluate the patient’s progress and address any concerns.
Potential Side Effects and Management
Methylprednisolone (Solu-Medrol) and prednisone, while effective, carry potential side effects. Monitor closely for increased blood sugar, especially if you have diabetes. Regular blood glucose checks are recommended. High blood sugar can manifest as increased thirst, frequent urination, and blurred vision. Address these symptoms immediately with your doctor to adjust medication or manage blood sugar levels.
Gastrointestinal Issues
Both medications can irritate your stomach lining, causing indigestion, heartburn, or ulcers. Take them with food or milk to minimize this. If you experience severe stomach pain, nausea, or vomiting, contact your doctor immediately. Prescription antacids or proton pump inhibitors might be necessary.
Fluid Retention and Hypertension
Solu-Medrol, in particular, can cause fluid retention, leading to swelling in your legs and ankles, and potentially raising your blood pressure. Regularly monitor your weight and blood pressure. Your doctor may prescribe diuretics to manage fluid retention and blood pressure.
Mood Changes and Insomnia
Prednisone, especially at higher doses, may cause mood swings, anxiety, insomnia, or even depression. Maintain a regular sleep schedule, engage in relaxing activities, and communicate openly with your doctor about any significant mood changes. Your doctor may recommend an additional medication if necessary.
Other Potential Effects
Rare but serious side effects include increased risk of infections, muscle weakness, bone thinning (osteoporosis), and cataracts. Report any unusual symptoms, like persistent fever or unusual bruising, promptly. Your doctor may recommend preventative measures, such as calcium and vitamin D supplements, to mitigate long-term effects.
Important Note
This information is not a substitute for professional medical advice. Always consult your doctor or pharmacist before starting or stopping any medication, and for any concerns about side effects. They can personalize a management plan based on your individual needs and health status.
When to Consult a Physician: Importance of Medical Guidance
Contact your doctor immediately if you experience severe allergic reactions, such as difficulty breathing or swelling of your face, lips, or tongue. Don’t delay seeking medical attention for these symptoms.
Schedule a doctor’s appointment if your symptoms worsen despite medication, or if new symptoms develop. This includes increased pain, persistent nausea, or significant changes in your overall health. Your physician can assess your condition and adjust your treatment plan accordingly.
Medication Interactions and Adjustments
Always inform your physician about all medications you are taking, including over-the-counter drugs, herbal supplements, and vitamins. This is especially critical when starting or changing medications like Solu-Medrol or oral prednisone. Potential drug interactions can significantly impact treatment efficacy and safety.
Monitoring Your Progress
Regular follow-up appointments with your physician allow for close monitoring of your treatment response. Blood tests may be necessary to assess your progress and adjust medication dosages as needed. Don’t hesitate to contact your doctor with any questions or concerns between appointments.
Specific Symptoms Requiring Immediate Attention
Seek immediate medical attention for signs of infection such as fever, chills, or persistent cough. These symptoms can be serious and require prompt medical evaluation and treatment. Delaying care can lead to complications.